
Bridging the gap between study outcomes and real-world results. Algorithm-driven management in a rural cardioMEMS population

HTML: 0
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Authors
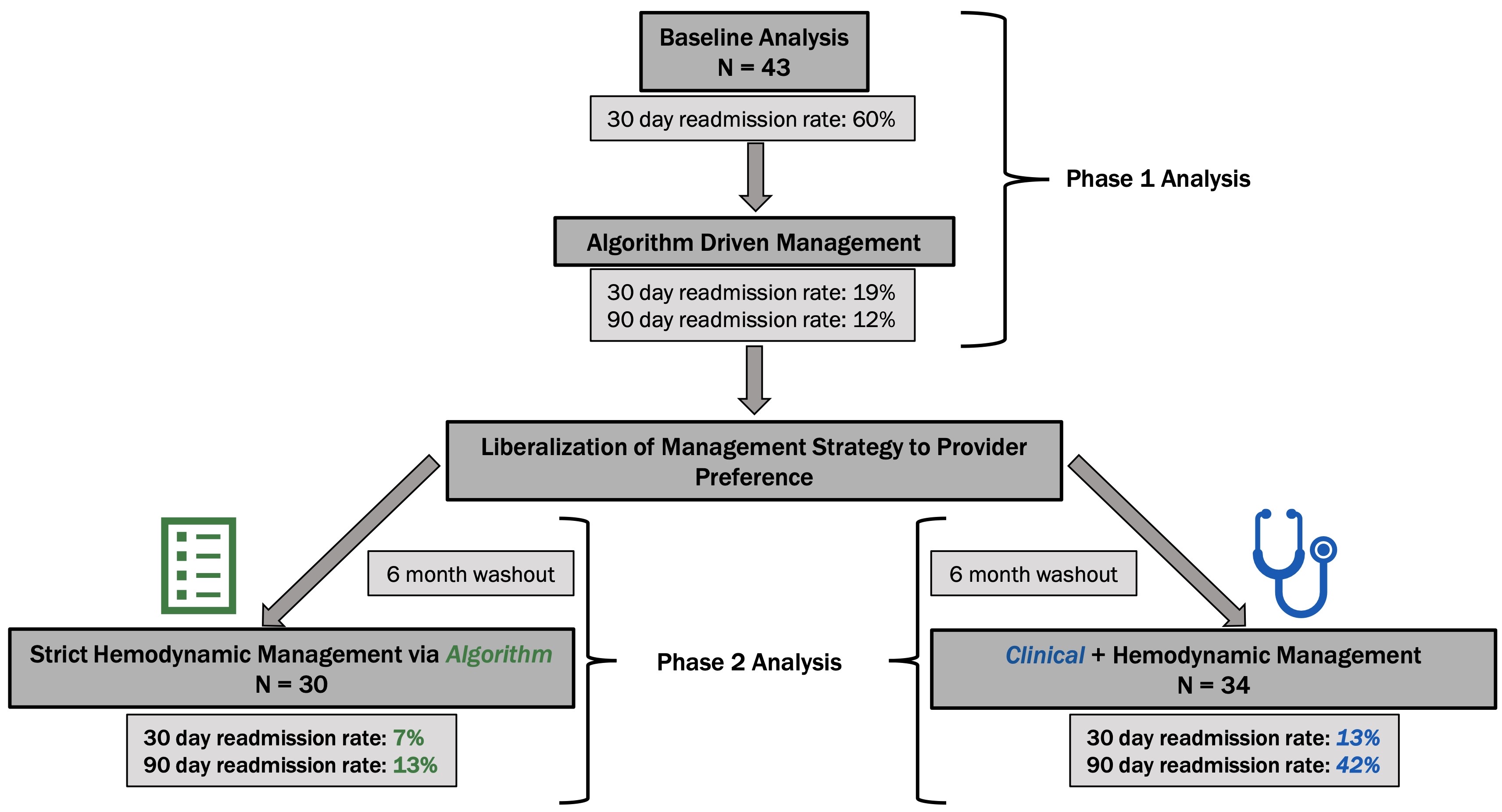
Current therapeutic strategies are ineffective at keeping heart failure patients out of hospital. In 2017, all-cause readmission rates were 19.9% at thirty-days and 34.6% at ninety-days. Large scale studies have shown potential advantages with remote pulmonary artery pressure monitoring. We sought to refine the management of our remotely monitored cohort by introducing a hemodynamic treatment algorithm. A population of rural heart failure patients previously implanted and managed with remote pulmonary artery pressure sensors were studied (n=43). Algorithm based hemodynamic management began with prospective outcome monitoring for ninety days during which algorithm use was mandatory. Following the initial observation period, some physicians reverted to prior practice habit which included consideration of standard heart failure metrics into decision making. Following a six-month washout period, retrospective analysis was performed in evaluation of the intervention arm (n=34), patients managed by hemodynamic plus usual heart failure data, and the control group (n=30), those who remained strictly managed by algorithm. Pre-algorithm thirty-day heart failure specific hospitalization (HFH) rate was 60%. Algorithm-driven management decreased HFH rates to 19% at thirty-days and 12% at ninety-days. Incorporating standard heart failure metrics with remotely pulmonary artery (PA) pressure data markedly increased risk of readmission (7% vs 13% at thirty-days and 13% vs 42% at ninety-days). Heart failure patients managed via remote pulmonary artery pressures benefitted from algorithm-driven hemodynamic therapies. Utility and effectiveness of remote PA monitoring is stunted with consideration of traditional heart failure metrics (weights, symptoms, exam findings) in their management.
Graphical Abstract
Altmetrics
Downloads
Citations




How to Cite

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
PAGEPress has chosen to apply the Creative Commons Attribution NonCommercial 4.0 International License (CC BY-NC 4.0) to all manuscripts to be published.



